
Vol 6 No 3 (2011)
Articles
-
Women die of cardiovascular disorders even more than a combination of breast cancer, stroke, chronic obstructive pulmonary disease, and lung cancer. Recent data show that while 1 out of 2.6 women die of coronary artery disease (CAD), only 1 out of 4.6 die from cancer. Whereas some studies show an increase in the age-adjusted mortality of CAD in both women and men, some other studies report an increase in mortality amongst young women. There is a significant decrease in sudden cardiac death in men without significant change in women, and more women die of CAD before their arrival at the emergency room of hospitals than do men. It is, therefore, regrettable that many women and their physicians are not sufficiently aware of the problem and this unawareness is believed to be a major culprit for the existing gender disparities and inaction on the part of women as regards risk modification. What is more, the bulk of our knowledge, preventive measures, diagnostic strategies, and treatment plans are on the basis of studies conducted chiefly in men, when powerful evidence-based gender-specific recommendations call for efforts to enroll more women in order to reach a desirable level of sex representation.
Given the significance of CAD assessment in women, it is essential that an acceptable risk score system be devised to estimate the risk of coronary events. The Framingham Risk Score, which has been used for this purpose for a long time, is no longer suitable for women and the Reynolds Risk Score seems to be a more appropriate tool.
Finally, from a pathophysiological point of view, endothelial and microvascular dysfunctions are the most salient contributors to the development of CAD in women by comparison with men and they give rise to non-obstructive CAD. Lamentably, most of the relevant studies conducted hitherto have focused predominantly on men; any attempt to redress the balance would be of great value in the endeavors to decrease the risk in women. -
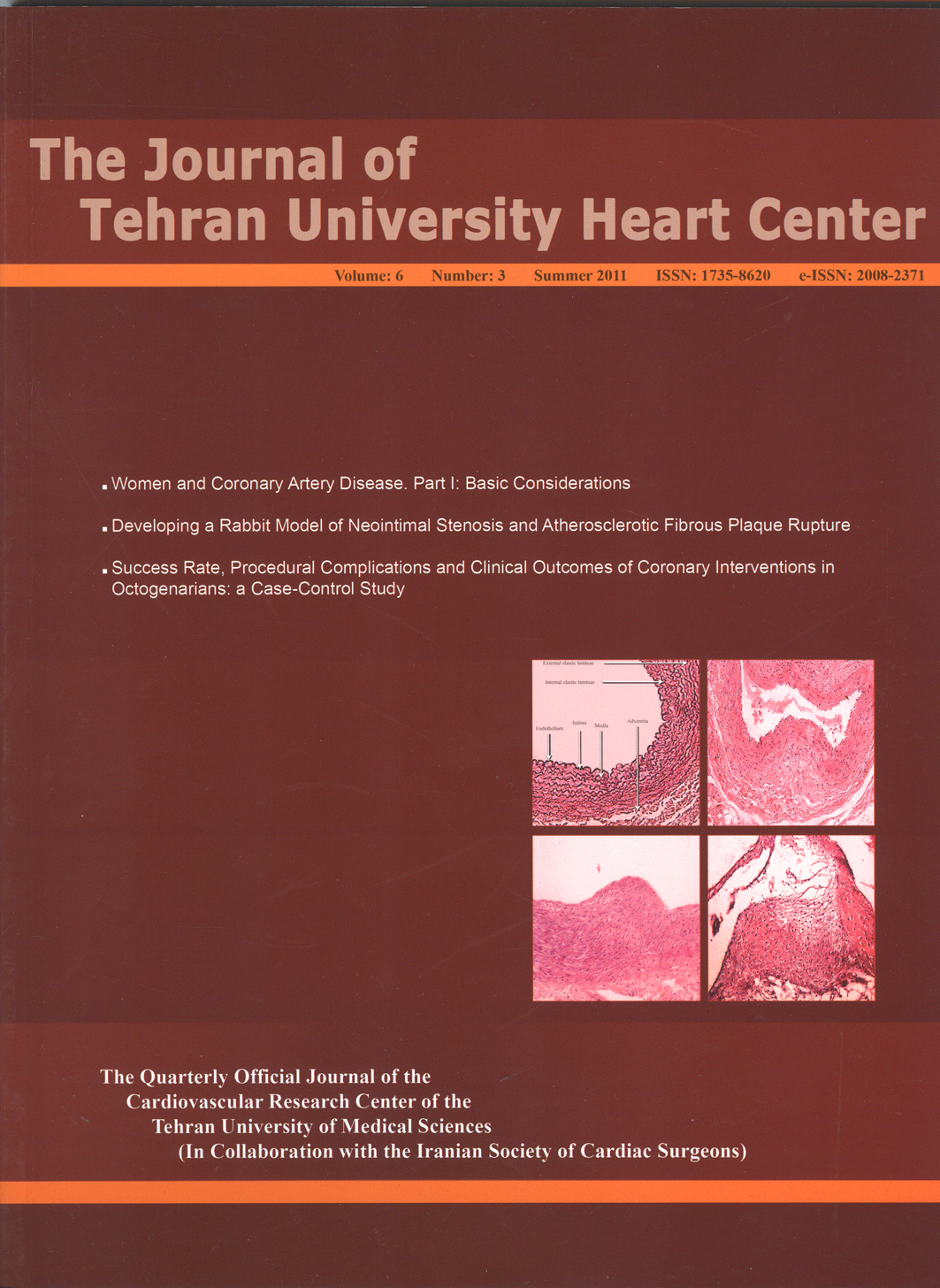
Background: A precise understanding of the mechanism of human neointimal stenoses and atherosclerotic fibrous plaques, which give rise to thromboses in vital arteries, requires a suitable animal model that would mimic the same characteristics well. We developed a rabbit model of neointimal stenosis and fibrotic plaque rupture in the carotid artery to visualize the lesion progress and to characterize the lesion types according to the American Heart Association classification.
Methods: Twenty-eight healthy male New Zealand white rabbits were randomly divided into two groups: The rabbits in group A (n = 14) consumed a standard chow diet, and those in group B (n = 14) were injured via perivascular cold injury using liquid nitrogen at the right common carotid artery before being fed a high cholesterol diet (1.5%) for eight weeks. Plasma lipid evaluation was performed before the sacrificing of the rabbits. At the end of every week, at least 1 rabbit from group B was sacrificed for an analysis of lesion histopathology and calculation of the area ratios of the intima to media.
Results: The plasma lipid level in group B was significantly higher than that in group A (p value < 0.05). The histopathological results revealed atherosclerosis characteristics such as endothelial layer destruction, fatty streaks and lipid-containing macrophages (foam cells) formation in the intima and media layers, extracellular lipid collections, smooth muscle cells proliferation and migration, neointima formation, intima thickening and deformation, fibrotic plaque formation, and finally plaque rupture. Statistical analysis revealed a significant increase in the intima-to-media ratio at the end of the eighth week (6.41 ± 0.27, p value < 0.05).
Conclusion: We successfully developed a rabbit model of neointimal stenosis and atherosclerotic fibrous connective tissue plaque rupture, which is not only quickly and easily reproducible and inexpensive but also without mortality. The merits of our model render the evaluation of neointimal stenoses and fibrotic plaques and their treatment strategies more feasible in humans. -
Background: Clinical trials of revascularization have routinely under-enrolled elderly subjects. Thus, symptom relief and improved survival might not apply to elderly patients, in whom the risk of mortality and disability from revascularization procedures seems to be high and co-morbidity is more prevalent. The present case control study was performed to draw a comparison in terms of the procedural success, procedural and in-hospital complications, and major adverse cardiac events (MACE) in a one-year follow-up of octogenarians (age ≥ 80 years) with a selected matched younger control group in the Tehran Heart Center Angioplasty Registry.
Methods: According to the Tehran Heart Center Interventional Registry of 9, 250 patients with a minimum follow-up period of one year between April 1993 and February 2010, 157 percutaneous coronary intervention (PCI) procedures were performed in 112 octogenarians. Additionally, 336 younger patients (459 PCI procedures) were selected from the database as the propensity-score matched controls.
Results: There were 147 (93.6%) and 441 (96.1%) successful PCI procedures in the elderly group and control group, respectively (p value = 0.204). Procedural complications were seen in 5 (3.2%) of the elderly group and 16 (3.5%) of the control group (p value = 0.858). Totally, 7 (6.3%) in-hospital complications occurred in the elderly group and 22 (6.8%) in the control group (p value = 0.866). One-year MACE was seen in 9 (9.1%) of the elderly and 18 (5.8%) of the control group (p value = 0.26).
Conclusion: Procedural success and complications, in-hospital complications, and one-year MACE were not significantly different between our two study groups. Therefore, age alone should not be used as the sole criterion when considering revascularization procedures. Furthermore, PCI should not be refused in octogenarians if indicated. -
Background: Coarctation of the aorta is a discrete stenosis of the proximal thoracic aorta. The common clinical pattern is congestive heart failure in infancy. Treatment methods include balloon angioplasty and surgical repair in this age group. Percutaneous balloon angioplasty is a less invasive method for the repair of discrete coarctation but remains controversial as a primary treatment strategy for a native coarctation. This study aimed to compare the effectiveness and outcome of balloon angioplasty and surgical repair in coarctation infants younger than 1 year old.
Methods: This retrospective study evaluated the results of the two methods in 167 patients younger than one year old admitted into a tertiary heart center pediatric ward with the diagnosis of coarctation of the aorta: Balloon angioplasty was done for 55 and surgical repair for 112 infants. Patients with previous interventions were not included in this study.
Results: Primary results revealed no significant difference in the effectiveness of the two methods (p value = 0.0601). While the rate of recurrent coarctation was significantly lower in the surgery group [19 (17%) vs. 11 (20%), p value = 0.0470], the mortality rate was lower in the balloon angioplasty method [5 (5.5%) vs. 13 (11.6%), p value = 0.039]. Our multivariate logistic regression model, however, showed no statistically significant difference (p value = 0.120).
Conclusion: Because of the incidence of re-coarctation, balloon angioplasty compared with surgical repair did not confer an improved outcome for our infants’ coarctation. -
Background: For all the wealth of research comparing the efficacy of the different types of the drug-eluting stent (DES) such as sirolimus- , paclitaxel- , and zotarolimus-eluting stents, there is still a dearth of data on the different brands of each DES type. We aimed to investigate the one-year clinical outcomes, including major adverse cardiac events (MACE), of the use of the ultra long Apollo paclitaxel-eluting stent in patients with long atherosclerotic coronary artery lesions.
Methods: According to a retrospective review of the Tehran Heart Center Registry of Interventional Cardiology, a single-center nonrandomized computerized data registry in which all adult patients who undergo single or multi-vessel percutaneous coronary intervention (PCI) are enrolled without any specific exclusion criteria, the mixed use of long Apollo paclitaxel-eluting stents and other types of the DES as well as myocardial infarction within forty-eight hours prior to the procedure was excluded. In total, 122 patients were enrolled in the study, and their baseline clinical, angiographic, and procedural characteristics were obtained. In addition, the patients’ follow-up data and, most importantly, MACE during a one-year period after intervention were recorded.
Results: The mean follow-up duration was 14.1 ± 3.8 months. The one-year clinical follow-up data were obtained in 95.9 % of all the patients. The incidence of MACE was 5.7% during the entire study period. There was 1 death, which occurred during the initial days after PCI. The incidence of non-fatal myocardial infarction was 2.5% (3 cases), including one patient who underwent target vessel revascularization seven months later. Also, 3 patients with single-vessel disease and in-stent restenosis underwent coronary artery bypass grafting between five to ten months later.
Conclusions: Our results showed that the Apollo paclitaxel-eluting stent might be regarded as a safe and effective treatment for long coronary lesions. -
Background: The optimal target for revascularization in patients with history of coronary artery bypass graft surgery (CABG) is unclear. This study was designed to compare the outcome of percutaneous coronary intervention (PCI) on saphenous vein grafts (SVG) and that on native vessels in patients with previous CABG in terms of major adverse cardiac events (MACE).
Methods: The study drew upon data on consecutive patients hospitalized for PCI and MACE rate during a nine-month follow- up period. The patients were divided according to the target vessel for PCI into two groups: SVG and native vessel.
Results: Between 2003 and 2007, 226 patients underwent PCI 6.57 ± 4.55 years after CABG. Their mean age was 59.52±9.38 years, and 176 (77.9%) were male. PCI was performed on the SVG in 63 (27.9%) patients and on the native coronary artery in the rest. During a nine-month follow-up period, 9 (4%) patients suffered MACE; the prevalence of MACE was not significantly different between the SVG group (4.8%) and the native vessel group (4.9%), (p value = 0.999).
Conclusion: PCI on grafted and native vessels did not affect MACE in patients undergoing PCI after CABG. -
The anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a rare congenital cardiac malformation. It presents predominantly in infancy and its main presenting feature is myocardial ischemia or heart failure. Survival to adulthood is quite uncommon. If untreated, mortality from ALCAPA approaches 90% in infancy; early recognition and surgical correction are, therefore, essential. With early surgical correction, the prognosis is good. There are two types of ALCAPA syndrome: the infant type and the adult type, each of which has different manifestations and outcomes. Infants experience myocardial infarction and congestive heart failure, and approximately 90% die within the first year of life. A literature review regarding this anomaly in teenagers and adults show that only 25 cases have been diagnosed during life and 18 additional cases of ALCAPA in these age groups have been diagnosed post mortem. We present a rare case of a 60-year-old man, who referred to our center due to dyspnea on exertion from the previous year without any history of chest pain and diagnosed as ALCAPA. Given the absence of ischemia and the patient’s age, only medical therapy was recommended.
-
We introduce a 32-year-old man who was evaluated for a dizziness and headache of unknown origin for at least two months and was referred to our center after ECG findings. He was finally diagnosed as a case of idiopathic, familial, diffuse, persistent atrial standstill, which is a rare arrhythmogenic condition characterized by the absence of electrical and mechanical activity in the atria. He successfully received a single-chamber permanent pacemaker.
-
Coronary revascularization in patients with dextrocardia is not a common clinical condition. There are very few cases of off-pump coronary artery bypass. A 64-year-old woman was admitted to a university hospital due to exertional chest pain. Her primary diagnosis was coronary artery disease superimposed on dextrocardia, which was first suspected on physical examination, with the patient having right-sided heart sounds on auscultation. It was corroborated by chest X-ray. After diagnostic evaluations, including coronary angiography, she underwent off-pump coronary artery bypass grafting due to a significant left main coronary artery stenosis associated with dextrocardia. Two years later, multi-slice CT angiography revealed patent grafts, demonstrating good clinical results.
-



