
Vol 5 No 4 (2010)
Articles
-
-
Atrial fibrillation (AF) is a commonly encountered arrhythmia in our daily practice. Every year a huge bulk of data is published about different management strategies, new antiarrhythmic drugs, anticoagulation protocols and ablation procedures in these patients. In this review article, we discuss different management strategies and new antiarrhythmic drugs as well as those commonly used. We will also have a brief look at anticoagulation in AF.
We try to introduce the most recent publications in this field and we think that this review article may not only give information about the current state of antiarrhythmic therapy of AF, it may also show some progresses that we may anticipate in the near future. New drugs are promising in the management of AF because of better safety profile and also acceptable efficacy. A comparison between the catheter ablation procedure and antiarrhythmic therapy is beyond the scope of this article.
-
Background: Ventriculoatrial (VA) conduction has an important role in the initiation and maintenance of some arrhythmias. The aim of this study was to evaluate whether clinical and electrophysiological parameters of atrioventricular (AV) conduction can predict VA conduction.
Methods: Detailed demographic, electrocardiographic, and echocardiographic data were recorded in 54 consecutive patients undergoing electrophysiological study for the evaluation of ventricular tachyarrhythmia. The basic parameters including atrial-His (AH) and His-ventricular (HV) intervals, atrioventricular Wenckebach point (AVWP), ventriculoatrial Wenckebach point (VAWP), anterograde effective refractory period of atrioventricular node(AERP-AVN), retrograde effective refractory period of atrioventricular node (RERP-AVN) and effective refractory period of ventricle (VERP) were measured based on standard protocol.
Results: Mean age of the patients was 59.4 (± 13.9) years. Forty-three (79.6%) patients were male and 39 (72.2%) had a history of ischemic heart disease. Ventriculoatrial (VA) conduction was recorded in 21 (38.9%) patients; it was slightly more prevalent in the men (44.2% vs. 18.2%; p value = 0.114). In the patients without VA conduction, the means of AVWP, AERP-AVN, and PR intervals were significantly more prolonged (p value = 0.007, 0.030, and 0.045, respectively), and a trend toward more prolonged AH, HV, and QRS interval was seen in them (p value = 0.078, 0.124, and 0.159, respectively). AVWP was the best predictor for the absence of Ventriculoatrial (VA) conduction. Fifty (92.5%) patients had a better AV than VA conduction. Age, presence of ischemic heart disease, left ventricular ejection fraction, and diastolic function could not predict VA conduction. A significant direct relationship was found between left ventricular ejection fraction and VAWP (p value = 0.036, r = 0.4; the Pearson correlation test).
Conclusion: Prediction of VA conduction based on clinical and echocardiographic characteristics is not possible. Impairment of AV conduction was the best predictor for the impairment of VA conduction, and most patients had a better AV than VA conduction. In this study, the men had a slightly higher prevalence of VA conduction. -
Background: Systolic blood pressure recovery (rSBP) is of prognostic value for predicting the survival and co-morbidity rate in patients with coronary artery disease (CAD). This study investigated the association between rSBP and exercise indices after complete cardiac rehabilitation program (CR) in a population-based sample of patients undergoing coronary artery bypass grafting (CABG).
Methods: The sample population consisted of 352 patients who underwent pure CABG. The patients underwent standard symptom-limited exercise testing immediately before and also after the completion of the CR sessions. rSBP was defined as the ratio of the systolic blood pressure at 3 minutes in recovery to the systolic blood pressure at peak exercise.
Results: An abnormal baseline rSBP after exercise was a strong predictor of exercise parameters in the last session, including metabolic equivalents (β = -0.617, SE = 0.127, p value < 0.001) and peak O2 consumption (β = -1.950, SE = 0.363, p value < 0.001) measured in the last session adjusted for baseline exercise characteristics, demographics, function class, and left ventricular ejection fraction.
Conclusion: The current study strongly emphasizes the predictive role of baseline rSBP after exercise in evaluating exercise parameters following CR. This baseline index can predict abnormal METs value, peak O2 consumption, post-exercise heart rate, and heart rate recovery after a 24-session CR program. -
Background: Carotid artery stenting is now used as an alternative to surgical endarterectomy. This study was done to assess the feasibility, safety, and immediate and late clinical outcomes in patients undergoing carotid stenting.
Methods: Between July 2008 and December 2009, a total of 40 patients (20 male, mean age: 65 ± 11 years, 19 symptomatic, and 90% high risk for endarterectomy) underwent carotid artery stenting with different embolic protection devices and carotid stents. Thirty-seven patients had coronary artery disease. Technical success rate, stroke/death/ myocardial infarction rate at 30 days, access-site complications, and contrast-induced nephropathy were assessed. For the evaluation of the influence of experience in carotid artery stenting on complications, the patients were divided into two groups: Group 1 included the first 20 treated patients and Group 2 comprised the remainder of the patients.
Results: The overall technical success rate was 100%. The cumulative in-hospital stroke death rate was 7.5% (n = 3: 2 deaths and 1 major stroke). Complications were more frequent in Group 1 (2/20, 10%; 2 deaths) than in Group 2 (1/20, 5%; 1 major stroke), but this was not statistically significant (p value = 0.09). No access-site complications occurred, and mild contrast-induced nephropathy occurred in 3 patients (7.5%). No major stroke or neurological deaths occurred during a mean follow-up of 12 months.
Conclusion: Carotid stenting seemed feasible and relatively safe in our experience. Advanced experience in carotid artery stenting appears to confer an acceptable peri-procedural stroke-death rate. -
Background: Although percutaneous coronary intervention (PCI) is an excellent therapy for coronary artery disease, there is a paucity of information on the efficacy of PCI in improving diastolic function, especially in Iran. Because of the high prevalence of left diastolic dysfunction in coronary artery disease patients and its probable progression to heart failure, an evaluation of the role of PCI in improving diastolic function is required.
Methods: Thirty patients scheduled for elective PCI were enrolled in this study providing that their systolic ejection fraction was > 40%. Before PCI and 48 hours and 3 months after PCI, echocardiography was done to evaluate some diastolic values in these patients.
Results: The mean age of all the patients was 54 ± 10 year, and 20 patients were male. All the patients had a low degree of left ventricular diastolic dysfunction. Isovolumic relaxation time (115 ± 10 before treatment versus 120 ± 1 and 119 ± 3 respectively 48 hours and 3 months after treatment), mitral E wave velocity in septal (0.70 ± 0.05 before treatment vs. 0.71 ± 0.15 and 0.72 ± 0.12 respectively 48 hours and 3 months after treatment), and the peak velocity of late filling due to atrial contraction (mitral A wave velocity) in septal (0.74 ± 0.02 before treatment vs. 0.73 ± 0.01 and 0.68 ± 0.16 respectively 48 hours and 3 months after treatment) showed improvement after PCI. It is notable that early diastolic mitral annulus velocity (E¢) wave velocity in the septal part of the mitral annulus improved significantly 48 hours and 3 months after PCI (p value < 0.05). The early-to-late diastolic tissue velocity ratio of the mitral annulus (E/A) ratio of the mitral inflow improved 48 hours after PCI; it was statistically significant (p value = 0.05). Also, mitral A wave velocity in septal and the E/A ratio of the mitral inflow improved significantly 3 months after PCI (p value < 0.05).
Conclusion: Improvement in some of values related to left ventricular diastolic function followed by PCI shows that this method can be used to improve cardiac diastolic function in patients with symptomatic coronary artery disease. -
Background: Transcatheter occlusion of the patent ductus arteriosus (PDA) is a minimally invasive treatment. The appropriate device size is chosen based on the angiographic measurement of the PDA. The current study aimed to assess the relationship between the transthoracic echocardiographic (TTE) measurements of the PDA prior to the occlusion procedure and the actual size of the deployed device.
Methods: We reviewed the available records of 7 patients (2 male) who underwent the procedure at our institution (mean age: 21 ± 12.7 years, range: 7 to 46 years). PDA closure was performed successfully using the Amplatzer Duct Occluder (n = 5) and its Chinese copycat, Cardi-O-Fix Occluder (n = 2).
Results: The TTE measurement of the aortic end diameter of the PDA showed a good linear regression correlation with the size of the implanted duct occluder [duct occluder size = 0.543 + (0.941× TTE measured diameter), R = 0.907; p value ≤ 0.01].
Conclusion: TTE can provide a good estimation of the size of the Amplatzer duct occluder. -
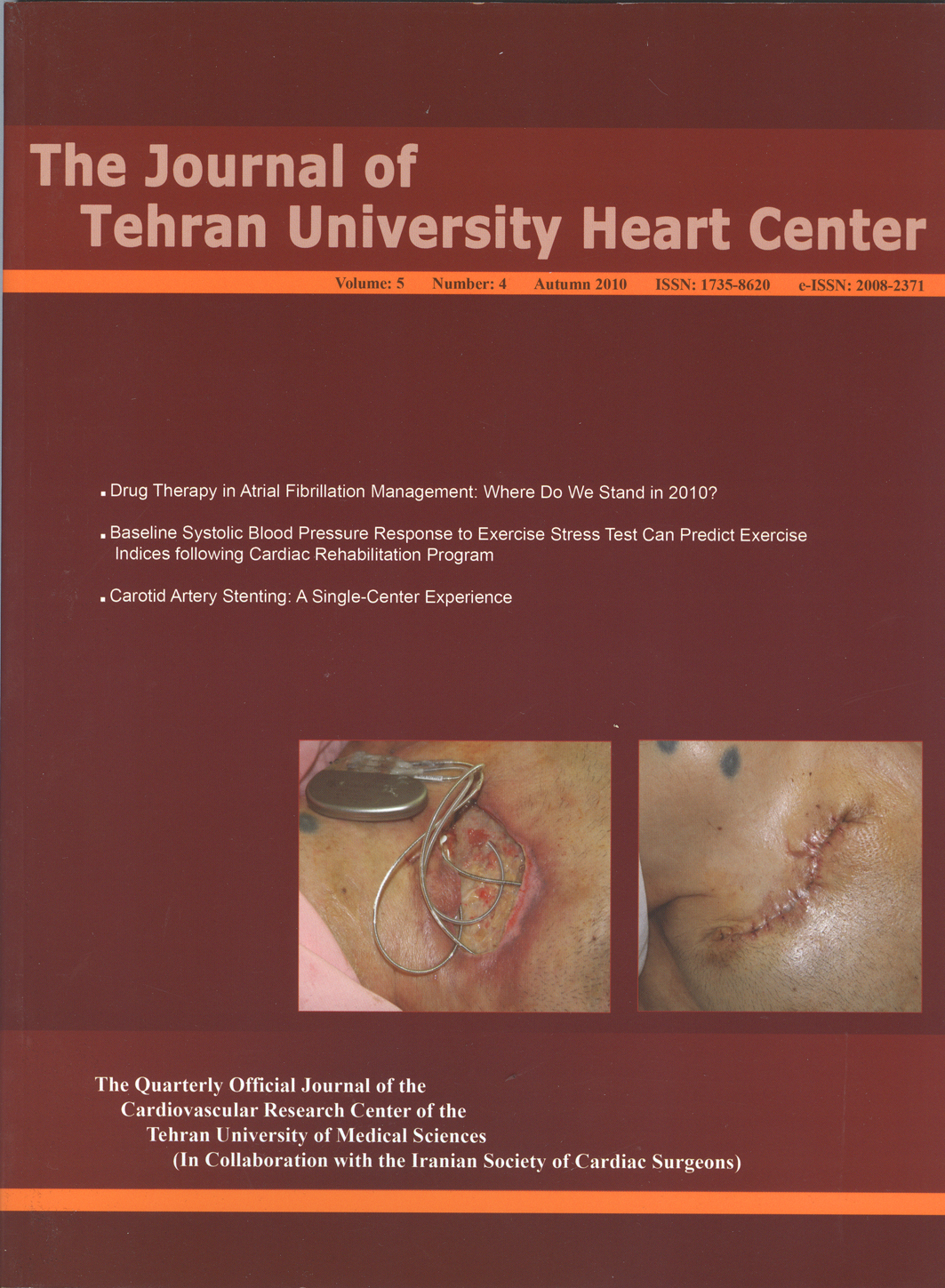
Pocket infection of a cardiac device is usually treated by removing the device and re-implanting it in a new site after complete treatment of the infection. This report illustrates a complicated case of pocket infection in the wake of the implantation of a permanent pacemaker (cardiac resynchronization therapy). The patient was treated conservatively through daily irrigation and dressing, broad-spectrum antibiotics, and debridement without the device being removed; the generator was kept out of the pocket for 5 weeks and then re-implanted in the same location successfully.
The method of treatment presented herein can be of value, not least in the elderly population who might experience life-threatening events following the replacement of their cardiac devices. -
There are many treatment modalities available to acutely terminate incessant ventricular tachycardia with variable success rates, but some cases tend to prove refractory to all of them. We report a 59-year-old woman presenting with incessant ventricular tachycardia. Echocardiography revealed a large true apical aneurysm and severe left ventricular dysfunction. The arrhythmia was controlled in the operating room after off-pump coronary artery bypass surgery and plication of the apical aneurysm.
-



