
Vol 17 No 4 (2022)
Review Article(s)
-
Background: To assess the cost-effectiveness of sacubitril/valsartan compared with enalapril in patients with heart failure with reduced ejection (HFrEF).
Methods: A systematic literature search was conducted searching in major electronic databases from inception to January 1, 2021. All relevant full economic evaluation studies of sacubitril/valsartan versus enalapril for the treatment of patients with HFrEF were identified using ad hoc search strategies. Mortality, hospital admissions, quality-adjusted life years (QALYs), life-years (LYQs), annual drug costs, total lifetime costs, and incremental cost-effectiveness ratio (ICER) were considered as the outcomes. The quality of the included studies was assessed using the CHEERS checklist. This study was conducted and reported in accordance with the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) guidelines.
Results: The initial search yielded a pool of 1026 articles, of which 703 unique articles were screened, 65 full-text articles were assessed for eligibility and 15 studies finally included in the qualitative synthesis. Studies show that sacubitril/valsartan reduces mortality and hospitalization rate. The mean of death risk ratio and hospitalization were computed at 0.843 and 0.844, respectively. Sacubitril/valsartan produced higher annual and total lifetime costs. The lowest and highest lifetime costs for sacubitril/valsartan were found in Thailand ($4,756) and Germany ($118,815), respectively. The lowest ICER was reported in Thailand ($4857/QALY) and the highest in the USA ($143,891/QALY).
Conclusion: Sacubitril/valsartan is associated with better outcomes and may be cost-effective compared to enalapril for the management of HFrEF. However, in developing countries such as Thailand, sacubitril-valsartan costs must be reduced to yield an ICER below the threshold.

Editorial
-
No Abstrac No Abstrac No Abstrac
Original Article(s)
-
Background: The trans-radial approach significantly reduces access bleeding and underlying vascular complications and is associated with lower healthcare costs than the transfemoral approach. One of the most common complications, however, is radial artery occlusion (RAO).
Methods: This study investigates the effects of verapamil on radial artery thrombosis in patients referred to Taleghani Hospital in Tehran between 2020 and 2021. Patients were randomized into 2 groups: the first group received verapamil, nitroglycerin, and heparin and the second group nitroglycerin and heparin. To randomly assign 100 cases to the 2 experimental and control groups, we first formed a framework for sampling 100 people (from 1 to 100); then, based on the table of random numbers, we assigned the first 50 numbers to the experimental group and the remainder to the control group. The 2 groups were compared for radial artery thrombosis.
Results: This study evaluated 100 candidates for coronary angiography in 2 groups of 50 with and without verapamil. The mean age was 58.6±11.2 years in the group with verapamil and 58.1±12.7 years in the group without verapamil (P=0.84). The difference between the 2 groups in terms of heart failure was statistically significant (P<0.028). The prevalence of clinical thrombosis was 2.0% in the group with verapamil and 22.0% in the group without verapamil (P<0.004). The prevalence of ultrasound-confirmed thrombosis was 4.0% in the group with verapamil and 36.0% in the group without verapamil (P<0.001).
Conclusion: Intra-arterial injection of verapamil added to heparin and nitroglycerine during trans-radial angiography could significantly reduce RAO.
-
Background: Compliance with health-related behaviors is a dilemma among heart failure (HF) patients. The present study aimed to assess the validity and reliability of a Persian translation of the revised heart failure compliance questionnaire (RHFCQ) in Iranian HF sufferers.
Methods: This methodological study was performed on outpatient HF individuals referred to a heart clinic in Isfahan, Iran. The forward-backward translation method was used for translation. Twenty subjects were invited to express their opinions on the provided items concerning simplicity and understandability. Twelve experts were invited to rate the items regarding the content validity index (CVI). Cronbach’s α was used to evaluate internal consistency. The patients were asked to complete the questionnaire for the second time after 2 weeks to investigate test-retest reliability using the intraclass correlation coefficient (ICC).
Results: There were no obvious difficulties during the translation and assessment of the simplicity and comprehensiveness of the questionnaire items. The CVI of the items ranged from 0.833 to 1.000. Totally, 150 patients (age: 64.60±15.00 y, males: 58.0%) filled in the questionnaire twice with no missing data. The highest and lowest compliance rates were attributed to alcohol and exercise domains, respectively (83.00±7.70% and 45.55±12.00%, respectively). Cronbach’s α was 0.629. After the omission of 3 items related to smoking and alcohol cessation, Cronbach’s α rose to 0.655. The ICC showed an acceptable value of 0.576 (95% CI, 0.462 to 0.673).
Conclusion: The modified Persian RHFCQ is a simple and meaningful tool with acceptable moderate reliability and good validity for assessing compliance in Iranian HF patients.
-
Background: We aimed to investigate the association between persistent early repolarization (ER) in healthy individuals and long-term cardiovascular events and mortality rates in a large cohort study.
Methods: Demographic characteristics, medical records, 12-lead electrocardiograms (ECGs), and laboratory data were retrieved and analyzed from the Isfahan Cohort Study. The participants were followed up biannually via telephone interviews and 1 live structured interview in between until 2017. Individuals who had ER in all their ECGs were considered persistent ER cases. Study outcomes were cardiovascular events (unstable angina, myocardial infarction, stroke, and sudden cardiac death), cardiovascular-related mortality, and all-cause mortality. The independent t test, the χ2 test, the Mann-Whitney U test, and the Cox regression models were used for statistical analyses.
Results: The study population consisted of 2696 subjects (50.5% female). Persistent ER was found in 203 subjects (7.5%), with a higher frequency in men (6.7% vs 0.8%; P<0.001). Cardiovascular events, cardiovascular-related mortality, and all-cause mortality occurred in 478 (17.7%), 101 (3.7%), and 241 (8.9%) individuals, respectively. After controlling for known cardiovascular risk factors, we found an association between ER and cardiovascular events (adjusted hazard ratio [95% confidence interval] =2.36 [1.19–4.68], P=0.014), cardiovascular-related mortality (4.97 [1.95–12.60], P=0.001), and all-cause mortality (2.50 [1.11–5.58], P=0.022) in women. No significant association was found between ER and any study outcomes in men.
Conclusion: ER is common in young men with no apparent long-term cardiovascular risks. In women, ER is relatively rare, but it could be associated with long-term cardiovascular risks.
-
Background: Coronary slow flow (CSF) is defined as decreased coronary blood circulation velocity and delayed opacification of contrast media during angiography. Evidence is insufficient regarding the course and prognosis of CSF patients. Long-term follow-up can help better understand the physiopathology and outcome of CSF. Accordingly, we assessed the long-term outcomes of CSF patients in this study.
Methods: This retrospective cohort study was carried out on 213 CSF patients consecutively admitted to a tertiary health care center from April 2012 through March 2021. After data collection from the patients’ files, follow-up was done via telephone call invitations and assessments of existing data in the outpatient cardiology clinic. The comparative analysis was conducted using a logistic regression test.
Results: The mean follow-up length was 66.26±15.32 months, 105 patients (52.2%) were male, and the mean age of the patients was 53.81±11.91 years. The left anterior descending was the main affected artery (42.8%). At long-term follow-up, 19 patients (9.5%) required repeated angiography. Three patients (1.5%) had a myocardial infarction and 5 (2.5%) died from cardiovascular etiologies. Three patients (1.5%) underwent percutaneous coronary intervention. No patient required coronary artery bypass grafting. The need for a second angiography had no association with sex, symptoms, and echocardiographic findings.
Conclusion: The long-term outcome of CSF patients is good, but their follow-up is necessary for the early diagnosis of cardiovascular-related adverse events.
-
Background: This study aimed to investigate the possible relationship between different stent sizes and clinical outcomes after percutaneous coronary intervention (PCI) in patients with diabetes treated with drug-eluting stents (DESs) and dual antiplatelet therapy (DAPT).
Methods: Patients with stable coronary artery disease undergoing elective PCI with the DES were entered into a retrospective cohort between 2003 and 2019. Major adverse cardiac events (MACE), defined as the combined endpoint of revascularization, myocardial infarction, and cardiovascular death, were recorded. The participants were categorized according to the stent size: 27 mm for length and 3 mm for diameter. DAPT (aspirin and clopidogrel) was used for at least 2 years for diabetics and 1 year for nondiabetics. The median duration of follow-up was 74.7 months.
Results: Out of 1630 participants, 29.0% had diabetes. The diabetics constituted 37.8% of those with MACE. The mean diameter of the stents in the diabetics and nondiabetics was 2.81±0.29 mm and 2.90±0.35 mm, respectively (P>0.05). The mean stent length was 19.48±7.58 mm and 18.92±6.64 mm in the diabetics and nondiabetics, respectively (P>0.05). After adjustments for confounding variables, MACE was not significantly different between the patients with and without diabetes. Although MACE incidence was not affected by stent dimensions in the patients with diabetes, the nondiabetic patients implanted with a stent length exceeding 27 mm experienced MACE less frequently.
Conclusion: Diabetes did not influence MACE in our population. Additionally, stents of different sizes were not associated with MACE in patients with diabetes. We propose that using the DES supplemented by long-term DAPT and tight control of glycemic status after PCI could decrease the adverse consequences of diabetes.
-
Background: Patients with cardiovascular disorders (CVD) are at higher risk for potential drug-drug interactions (pDDIs) due to complex treatment regimens. This study aimed to evaluate pDDI patterns in physicians’ prescriptions in a specialized heart center using simple software.
Methods: This cross-sectional study identified severe and related interactions during a 2-stage survey of experts. The data collected included age, sex, the date of admission and discharge, the length of hospital stay, drug names, inpatient wards, and the final diagnosis. The extracted drug interactions were used as a source of software knowledge. The software was designed using the SQL Server and the C # programming language.
Results: Of 24 875 patients included in the study, 14 695 (59.1%) were male. The average age was 62 years. Based on the survey of experts, only 57 pairs of severe pDDIs were identified. The designed software evaluated 185 516 prescriptions. The incidence of pDDIs was 10.5%. The average number of prescriptions per patient was 7.5. The highest frequency of pDDIs was detected in patients with diseases of the lymphatic system (15.0%). Aspirin with heparin (14.3%) and heparin with clopidogrel (11.7%) were the most common documented pDDIs.
Conclusion: This study reports the prevalence of pDDIs in a cardiac center. Patients with lymphatic system disorders, male patients, and older patients were at higher risk of pDDIs. This study shows that pDDIs are common among CVD patients and highlights the need to use computer software to screen patients’ prescriptions to assist in detection and prevention.
-
Target: Bendopnea, defined as dyspnea while bending, can be observed in patients with heart failure (HF). In this study, we investigated the frequency of this symptom in patients with systolic HF and its association with echocardiographic parameters.
Material and Methods: In this study, patients with left ventricular ejection fraction (LVEF) ≤45% and decompensated HF referred to our clinics were prospectively recruited. All patients were examined by cardiologists for collecting data on the presence of bendopnea and baseline characteristics. They also underwent electrocardiographic and echocardiographic examinations. All findings compared between patients with or without bendopnea.
Results: A total of 120 patients with a mean age of 65.19 ± 12.62 years were evaluated, and 74.8% were men. Bendopnea was observed in 44.2% of the patients. The etiology of HF was ischemic in most patients (81.9%), and the functional class of most patients (85.9%) was III or IV. The mortality rate at 6 months follow-up was comparable between patients with or without bendopnea (6% vs. 9.5%, p=0.507). The waist circumference (odds ratio [OR] 1.037, 95% confidence interval [CI] 1.005 – 1.070, p = 0.023), paroxysmal nocturnal dyspnea (OR 0.338, 95% CI 0.132 – 0.866, p = 0.024), and right atrium size (OR 1.084, 95% CI 1.002 – 1.172, p = 0.044) were associated with bendopnea.
Conclusions: Bendopnea can be frequently found among patients with systolic HF. This phenomenon is associated with obesity and baseline symptoms of patients and right atrium size upon echocardiographic examinations. It can help clinicians with the risk stratification of HF patients.
-
Background. This study aimed to investigate readmission risk factors after ST-elevation myocardial infarction (STEMI) during a 3-year follow-up.
Methods: This study is a secondary analysis of the STEMI Cohort Study (SEMI-CI) in Isfahan, Iran, with 867 patients. A trained nurse gathered the demographic, medical history, laboratory, and clinical data at discharge. Then the patients were followed up annually for 3 years by telephone and invitation for in-person visits with a cardiologist concerning readmission status. Cardiovascular readmission was defined as MI, unstable angina, stent thrombosis, stroke, and heart failure. Adjusted and unadjusted binary logistic regression analyses were applied.
Results: Of 773 patients with complete information, 234 patients (30.27%) experienced 3-year readmission. The mean age of the patients was 60.92±12.77 years, and 705 patients (81.3%) were males. The unadjusted results showed that smokers were 21% more likely to be readmitted than nonsmokers (OR, 1.21; P=0.015). Readmitted patients had a 26% lower shock index (OR, 0.26; P=0.047), and ejection fraction had a conservative effect (OR, 0.97; P<0.05). The creatinine level was 68% higher in patients with readmission. An adjusted model based on age and sex showed that the creatinine level (OR, 1.73), the shock index (OR, 0.26), heart failure (OR, 1.78), and ejection fraction (OR, 0.97) were significantly different between the 2 groups.
Conclusion: Patients at risk of readmission should be identified and carefully visited by specialists to help improve timely treatment and reduce readmissions. Therefore, it is recommended to pay special attention to factors affecting readmission in the routine visits of STEMI patients.
-
Background: The aim of this study was to investigate the association between the platelet/lymphocyte ratio (PLR) and the neutrophil/lymphocyte ratio (NLR) and postoperative atrial fibrillation (POAF) after lung resection.
Methods: After the implementation of the exclusion criteria, 170 patients were retrospectively analyzed. PLR and NLR were obtained from fasting complete blood counts before surgery. POAF was diagnosed using standard clinical criteria. The associations between different variables and POAF, NLR, and PLR were calculated using univariate and multivariate analyses. The receiver operating characteristics (ROC) curve was used to determine the sensitivity and specificity of PLR and NLR.
Results: Of the 170 patients, 32 with POAF (mean age =71.28±7.27 y, 28 males and 4 females) and 138 patients without POAF (mean age =64.69±10.31 y, 125 males and 13 females) were identified, and the difference in the mean age was statistically significant (P=0.001). It was found that PLR (157.67±65.04 vs 127.52±56.80; P=0.005) and NLR (3.90±1.79 vs 2.04±0.88; P=0.001) were statistically significantly higher in the POAF group. In the multivariate regression analysis, age, lung resection size, chronic obstructive pulmonary disease, NLR, PLR, and pulmonary arterial pressure were independent risk factors. In the ROC analysis, PLR had a sensitivity of 100% and a specificity of 33% (AUC, 0.66; P<0.001), and NLR had a sensitivity of 71.9% and a specificity of 87.7% (AUC, 0.87; P<0.001). A comparison of AUC between PLR and NLR showed that NLR was statistically more significant (P<0.001).
Conclusion: This study showed that NLR was a stronger independent risk factor than PLR for the development of POAF after lung resection.
-
Background: Uncontrolled hypertension is a major public health problem among patients in developed and developing countries. The present study was conducted to investigate the prevalence and causes of uncontrolled hypertension to facilitate the design of more effective methods of hypertension control.
Methods: This cross-sectional study was conducted on 303 adults with hypertension. The Standard Health Literacy Questionnaire was used to collect data. Uncontrolled hypertension was ascertained based on the WHO definition. A multiple logistic regression model was used at a 95% confidence level. Variables considered were confounders including age, sex, marital status, family size, income (monthly mean), smoking (past or current), education level, and physical activity (times in a week).
Results: The mean (SD) age of the participants (n=303) was 59.3(12.7) years, and 57.4% were men. The prevalence of uncontrolled hypertension was 50.5%. The mean score of health literacy among patients with controlled hypertension was higher than that among patients with uncontrolled hypertension (64.83±23.72 vs 46.28±22.19; P<0.001). The odds of uncontrolled hypertension decreased by 3% in the patients (OR: 0.97; P=0.06). Adherence to treatment (OR: 0.13; P<0.001), salt consumption per package purchased per month (OR: 4.40; P=0.001), increased physical activity per hour per week (OR: 0.56; P<0.001), current or passive cigarette smoking (OR: 4.59; P=0.010), a positive history of chronic diseases (OR: 2.62; P=0.027), and increased family size (per 1 child) (OR: 0.57; P<0.001) were associated with uncontrolled hypertension.
Conclusion: The results showed a borderline association between increased health literacy and hypertension control. Additionally, increased salt consumption, reduced physical activity, small family size, and underlying diseases (eg, diabetes, chronic heart disease, and renal disease) could increase the odds of uncontrolled hypertension in Iranian society.
Case Report(s)
-
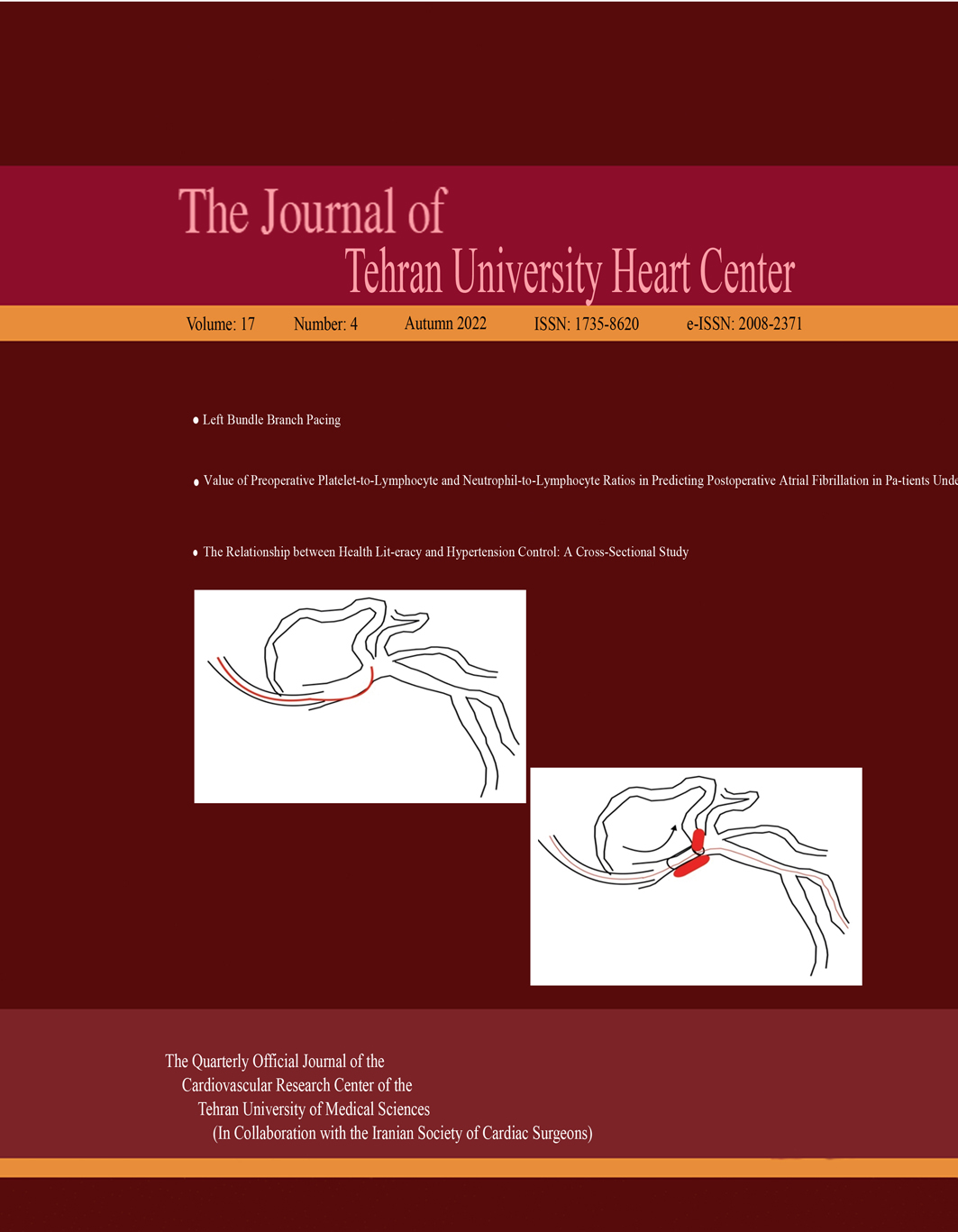
Coronary artery perforations and dissections, associated with cardiac tamponade or acute vessel closure, are life-threatening complications of percutaneous coronary intervention. In some cases, subepicardial hematomas could occur and compress the vessel. A 59-year-old woman was admitted to our hospital with chest pain and was diagnosed with non–ST-elevation myocardial infarction. Coronary angiography showed the total occlusion of the diagonal artery. During the intervention, left main coronary artery dissection and intramural hematoma occurred as coronary complications. The left main coronary artery was stented; however, the extension of the hematoma through the ostium of the left anterior descending artery caused further complications. The patient underwent an urgent coronary artery bypass graft surgery and was discharged on the seventh postoperative day.
Letter to the Editor
-
Background: Diabetic ketoacidosis (DKA) can cause several complications. The myocardial damage in children with DKA was not evaluated clearly. This study aimed to investigate the troponin level as a biochemical marker of myocardial damage in children with DKA during the disease and after recovery.
Methods: This cross-sectional study was conducted in the pediatric endocrinology department of Namazi Hospital, Shiraz, Iran, from May to December 2019. Fifty diabetic children aged 1 to 18 years old with DKA by census sampling method. All patients were examed, and electrocardiography (ECG) was carried out. Troponin level was measured at admission and 48 hours after recovery. Finally, data were analysed using SPSS software 20.
Results: At the time of admission, the mean troponin level was 11.56±5.35 ng/mL and it became 2.15±1.21 ng/mL after recovery. Although the initial troponin level during DKA in three patients was higher than the expected normal reference range, their echocardiography and ECG were normal. Moreover, there was no statistical relationship between troponin level with age, diabetes duration, and DKA severity.
Conclusion: The troponin level was remarkably different during DKA and after recovery. However, in merely 6% of DKA patients, the troponin level was higher than the expected value. We recommended that these patients be followed for future cardiovascular complications.
-
The present letter to editor comments the manuscript “Energy Drink-Associated Cardiomyopathy after Excessive Consumption: A Case Report. J Teh Univ Heart Ctr 2021;16(3):119-122” presenting some comments on consumption of energy drinks and cardiac damages.



