
Vol 15 No 2 (2020)
Original Article(s)
-
Background: Ankylosing spondylitis (AS) is a chronic inflammatory condition associated with more cardiac manifestations than those in the normal population. In this study, we sought to determine the prevalence of cardiac involvement in patients suffering from AS without cardiovascular risk factors.
Methods: The present case-control study, conducted in 2 university hospitals in Tehran from January 2016 to December 2017, recruited 67 patients with AS and 40 age- and sex-matched healthy controls. The diagnosis of AS was based on the classification criteria of the Assessment of SpondyloArthritis International Society. All the participants were examined using transthoracic echocardiography and a standard 12-lead ECG. Baseline characteristics, echocardiographic findings, and ECG features were compared between the AS and control groups using univariate analyses.
Results: The median age was 33.5 (IQR25-75%: 20.5–59) years in the AS group and 35 (IQR25-75%: 26–59) years in the control group (P=0.301). The number of patients with left ventricular systolic and diastolic dysfunction was significantly higher in the patients with AS than in the controls (7.5% vs. 20.9%; P=0.067, and 22.9% vs. 5.0%; P=0.026, respectively). The number of individuals with a left-axis deviation and a left anterior fascicular block was significantly higher in the patients suffering from AS than in the control group. The number of patients with aortic valve involvement was comparable between the groups (P=0.332).
Conclusion: The most common cardiac involvement in our patients with AS was left ventricular dysfunction, followed by rhythm disturbances and aortic valve insufficiency. These findings were independent of age, AS severity, and disease duration. Therefore, the implementation of cardiovascular screening can be recommended for patients with AS. -
Background: No-reflow is a major challenging issue in the management of patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PPCI). This study aimed to investigate the clinical, laboratory, and procedural predictors of no-reflow.
Methods: This study was conducted on 378 patients with STEMI admitted to Dr. Heshmat Educational and Remedial Center (a referral heart hospital in Rasht, Iran) between 2015 and 2017. The study population was divided based on the thrombolysis in myocardial infarction (TIMI) flow grade and the myocardial blush grade into no-reflow and reflow groups. The clinical, laboratory, and procedural characteristics at admission were compared between the 2 groups using the multivariate logistic regression analysis.
Results: The mean age of the participants was 58.57±11.49 years, and men comprised 74.1% of the study population. The no-reflow phenomenon was found in 77 patients. The no-reflow group was significantly older and more likely to be female; additionally, it had higher frequencies of hypertension, diabetes mellitus, hyperlipidemia, and a history of cardiovascular diseases. The multivariate logistic regression analysis showed that age >60 years (OR=1.05, 95% CI:1.00–1.09), hypertension (OR=2.91, 95% CI:1.35–6.27), diabetes (OR=4.18, 95% CI:1.89–9.22), a low systolic blood pressure (OR=3.53, 95% CI:1.02–12.2), a history of cardiovascular diseases (OR=4.29, 95% CI:1.88–9.77), chronic heart failure (OR=4.96, 95% CI:1.23–20), a low initial TIMI flow grade (OR=7.58, 95% CI:1.46–39.2 ), anemia (OR=3.42, 95% CI:1.33–8.77), and stenting vs. balloon angioplasty (OR=0.42, 95% CI:0.19–0.91) were the significant independent predictors of no-reflow.
Conclusion: This study revealed some clinical, laboratory, and procedural predictors of no-reflow for the prediction of high-risk patients and their appropriate management to reduce the risk of no-reflow. -
Background: In patients with heart failure, elevated levels of blood urea nitrogen (BUN) is a prognostic factor. In this study, we investigated the prognostic value of elevated baseline BUN in short-term mortality among patients with acute pulmonary embolism (PE).
Methods: Between 2007 and 2014, cardiac biomarkers and BUN levels were measured in patients with acute PE. The primary endpoint was 30-day mortality, evaluated based on the baseline BUN (≥14 ng/L) level in 4 groups of patients according to the European Society of Cardiology’s risk stratification (low-risk, intermediate low-risk, intermediate high-risk, and high-risk).
Results: Our study recruited 492 patients with a diagnosis of acute PE (mean age=60.58±16.81 y). The overall 1-month mortality rate was 6.9% (34 patients). Elevated BUN levels were reported in 316 (64.2%) patients. A high simplified pulmonary embolism severity index (sPESI) score (OR: 5.23, 95% CI: 1.43–19.11; P=0.012), thrombolytic or thrombectomy therapy (OR: 2.42, 95% CI: 1.01–5.13; P=0.021), and elevated baseline BUN levels (OR: 1.04, 95% CI: 1.01–1.03; P=0.029) were the independent predictors of 30-day mortality. According to our receiver-operating characteristics analysis for 30-day mortality, a baseline BUN level of greater than 14.8 mg/dL was considered elevated. In the intermediate-low-risk patients, mortality occurred only in those with elevated baseline BUN levels (7.2% vs. 0; P=0.008).
Conclusion: An elevated baseline BUN level in our patients with PE was an independent predictor of short-term mortality, especially among those in the intermediate-risk group. -
Background: Children with mitral valve prolapse (MVP) may be prone to ventricular arrhythmias due to transmural dispersion of repolarization (TDR). This study aimed to assess alterations in ventricular repolarization in children with MVP and to investigate their relationships with the degree of mitral regurgitation.
Methods: Fifty children with MVP and 50 age- and sex-matched healthy children as controls were studied. Twelve-lead electrocardiography and echocardiography were performed in all the subjects. TDR parameters were QT and QTc intervals, QTc dispersion, Tp-e interval, Tp-e interval dispersion, Tp-e/QT, Tp-e/QTc, JTc, JTc dispersion, Tp-e/JT, and Tp-e/JTc.
Results: The mean age of the 50 patients with MVP was 12.45±2.50 years (F/M: 15/35). There were no significant differences in QT and QTc intervals between the 2 groups. QTc dispersion (P=0.001), Tp-e dispersion interval (P=0.002), Tp-e/QTc (P=0.001), JTc dispersion (P=0.023), Tp-e/JT (P=0.004), and Tp-e/JTc (P=0.002) were significantly higher in the patients with MVP than in the healthy controls. Positive correlations were found between Tp-e dispersion interval and Tp-e/QTc and an increase in the degree of mitral regurgitation (P=0.012, r=0.42 and P=0.004, r=0.31, respectively). Additionally, positive correlations were detected between JTc dispersion and Tp-e/JTc and an increase in the degree of mitral regurgitation (P=0.032, r=0.20 and P=0.024, r=0.42, correspondingly).
Conclusion: In this study, TDR was damaged in children with MVP and was positively correlated with an increase in the degree of mitral regurgitation. It appears that children with MVP are prone to life-threatening ventricular arrhythmias.

Case Report(s)
-
Saphenous vein grafts (SVGs) are widely used conduits for the surgical revascularization of coronary arteries, but they are associated with poor long-term patency rates. Acute SVG thromboses often present as acute coronary syndrome and have an extensive atherosclerotic and thrombotic burden. Percutaneous coronary intervention (PCI) is the first treatment option; however, it carries a high risk of distal embolization, no-reflow, and periprocedural myocardial infarction. Reducing the thrombus burden and preventing distal embolization during PCI can be achieved by using some pharmacological strategies (e.g., glycoprotein IIb/IIIa antagonists) and devices (e.g., thrombectomy and filter devices). There are yet no better therapeutic options for patients undergoing PCI of SVG occlusions. Here, we introduce a 52-year-old male patient admitted with a typical acute chest pain of 1 hour’s duration. Electrocardiography showed signs of acute inferoposterior myocardial infarction. A thrombotic SVG occlusion was detected in primary PCI, and a huge thrombus content was aspirated. After the thrombus aspiration with stent therapy, the chest pain was relieved and the ST-segment elevation was improved. The patient has been followed without any symptoms for 10 months.
-
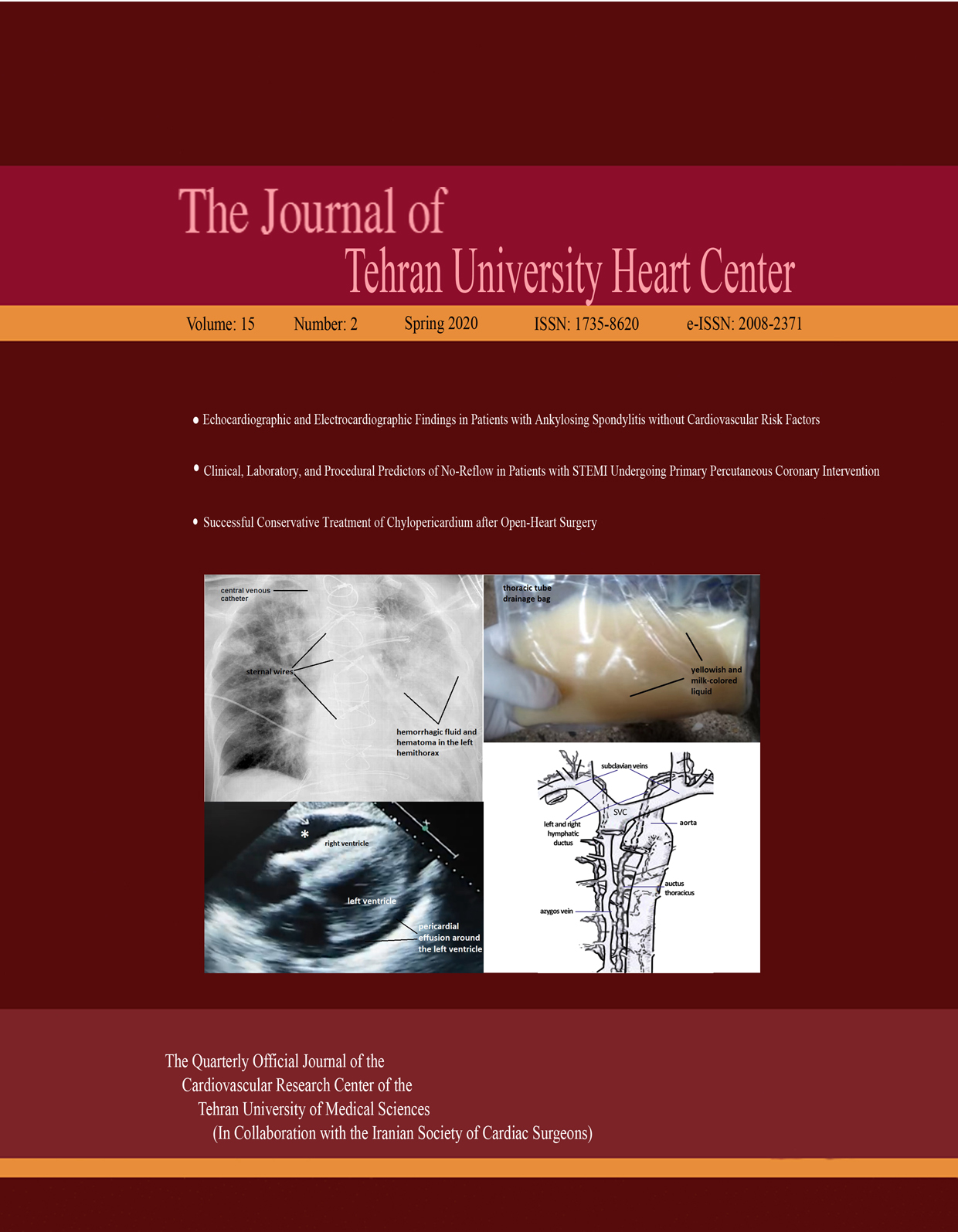
Chylopericardium is a rare complication following cardiac surgery. The incidence of this pathological condition is very low and mainly attributed to lymphatic injuries to the thymus or anterior mediastinum, thoracic duct injuries, or extensive posterior pericardial dissection with the possible interruption of major cardiac lymph channels.
A 62-year-old man was admitted to the cardiovascular surgery department for coronary bypass surgery, and the surgical procedure was performed 3 days later. Revision surgery was performed, because of the drainage associated with bleeding. In the post-revision days, the amount of serous drainage increased, and then chylous drainage occurred. After conservative treatment, the drainage of the chylous features decreased and eventually disappeared. The patient was discharged without any problem. At 6 months’ follow-up, the patient was doing well with a normal left ventricular function and without effusion. -
Percutaneous balloon mitral valvuloplasty (PBMV) has recently become the treatment of choice for many patients suffering from mitral stenosis. In the current report, we introduce a 26-year-old woman who presented to us with palpitation and exertional dyspnea but without any remarkable medical history. ECG illustrated the sinus rhythm, transthoracic echocardiography (TTE) showed severe rheumatic mitral stenosis and (2+) mitral regurgitation, and transesophageal echocardiography (TEE) demonstrated severe mitral stenosis and no thrombus. Accordingly, the patient underwent percutaneous transvenous mitral commissurotomy (PTMC). On the following day, TTE showed a fresh mobile thrombus in the right atrium attached to the atrial septum, which was confirmed by TEE. As a result, the patient received 1 mg/kg (60 mg) of enoxaparin subcutaneously twice daily plus 5 mg of warfarin daily. Subsequent TTE revealed no mass 4 days after the treatment. Evidence suggests that endocardial surface injury and trans-septal puncture during PTMC may be associated with clot formation, which is aggravated by low blood flow in the right atrium and the catheter as a foreign body. This case report emphasizes the importance of post-PTMC anticoagulant therapy.
-
The sternal foramen is an anatomical variation at the lower third of the sternum which carries the risk of life-threatening complications such as pneumothorax. It is usually asymptomatic and can be misinterpreted as an acquired lesion. The sternum is close to the mediastinal structures; the sternal foramen, thus, leaves the lung, heart, and great vessels unprotected during invasive procedures. A 61-year-old male patient was admitted to our emergency department with sudden-onset chest pain. Acute coronary syndrome was diagnosed by the cardiology department. Coronary angiography confirmed the diagnosis of coronary artery disease, and the patient underwent urgent coronary artery bypass grafting. During the exploration, sternotomy was performed with a proper incision. Two sternal images were obtained via the median incision, and a sternal foramen was detected intraoperatively. To the best of our knowledge, this is the first case of sternotomy to undergo open-heart surgery for coronary heart disease and to be diagnosed with the sternal foramen intraoperatively. It is of vital importance that surgeons and interventionists recognize the sternal foramen, which leaves the mediastinal structures unprotected, and take early precautions.
-
Warfarin- induced spontaneous breast hematoma is a very rare disease, with only a few cases having been reported in the literature so far. We describe an 80-year-old woman who had warfarin therapy due to deep vein thrombosis in a lower extremity. The patient was admitted with a history of swelling and red area on her bilateral breasts, chest wall, right arm, and right flank. She was treated conservatively with success. She was discharged after about 3 weeks without complications and was well at 6 months’ follow-up.
Letter to the Editor
-
-



